Last week the US Food and Drug Administration released new warnings about the use of statins for patients in the United States. The warnings that have been added to labels in the US come from worries about liver injury, memory-loss and confusion, increased blood sugar levels and some new potentially dangerous interactions between one statin (lovastatin) and a range of other drugs.
Statins are used to inhibit the production of cholesterol in the body. The leading drug in the class, atorvastatin (Lipitor, from Pfizer) is the most-commonly prescribed drug in the world. In the last financial year in Australia, this drug alone cost the government AUD$637M. More than 14 out of every 100 people in Australia were taking a statin each day.
These are a class of drugs that have been around for a long, long time. Simvastatin, one of the oldest in the class, was first approved in the United States more than twenty years ago. So why are new restrictions being put on the labels of the statins now? And shouldn’t the public have been warned about these safety issues a long time ago?
It’s easy to blame the pharmaceutical industry for the problems given previous problems in marketing, conflicts of interest and illegal behaviour but of course the reality is always muddier and more difficult to understand than we’d like it to be. The reality is that the funding of clinical trials and the influence of industry in trial design is a spectrum – and there are different problems all the way along.
Along with some friends, I recently published a paper in Clinical Pharmacology & Therapeutics about clinical trials for antihyperlipidemics.
My friends were colleagues from my own centre, from St Vincent’s Hospital, the Children’s Hospital Informatics Program in Boston, and the Hospital for Sick Kids in Toronto. In the paper, we looked at all the trials that have been registered for these drugs on clinicaltrials.gov since 2007. Some of these trials had already been completed, some were underway, and some were still recruiting. The different patterns of trials funded by industry and non-industry tell an interesting story about the different agendas.
And there were some surprising results.
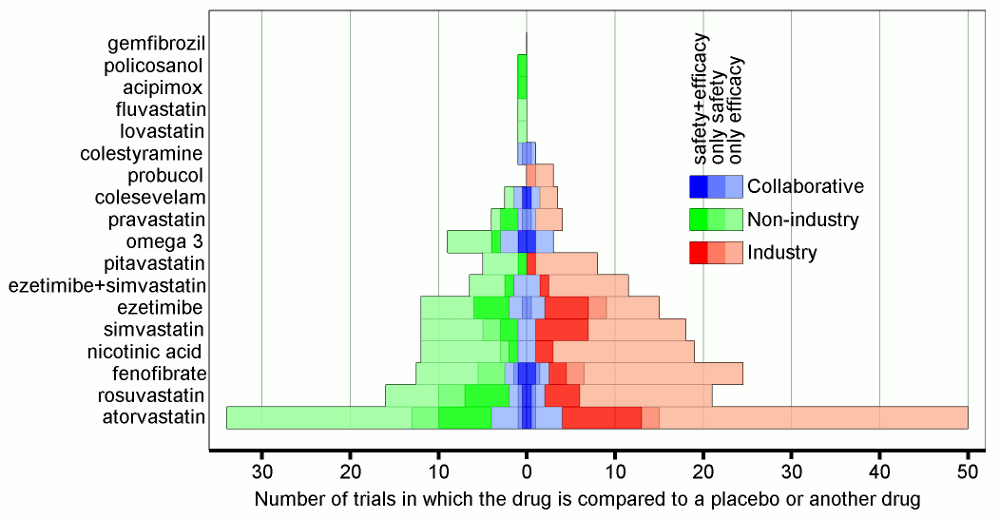
Trials funded by industry were (and are) typically larger and completed more quickly. They are also more likely to focus on hyperlipidemia rather than cardiovascular outcomes, and less likely to measure safety-related outcomes. The suprise was that industry-funded trials were more likely to register trials that directly compare two or more drugs.
This is a surprise because studies looking at publications of clinical trials find exactly the opposite – that published industry-funded clinical trials are less likely to compare between drugs. This gives us a pretty good hint about which of the trials are being undertaken and then not published.
The next surprise was that industry and non-industry trials had very similar patterns when it came to choosing which drugs to include in trials. Despite some specific differences in the choice of drugs, publicly-funded trials were just as unevenly distributed towards statins and atorvastatin in particular, and even more likely to test a drug against a placebo instead of another drug.
The work suggests or confirms the need to answer the following questions about clinical research in the area of cardiovascular risk and hyperlipidemia in particular:
- Why isn’t the pharmaceutical industry compelled to measure safety outcomes more often in clinical trials?
- What happens to the data from the comparative effectiveness trials undertaken by the pharmaceutical industry when they aren’t published?
- Why aren’t public funds directed more aggressively towards comparative effectiveness research, and towards interventions for which there isn’t already a glut of clinical trials being undertaken?
I think we need to be monitoring the clinical trials registries more closely when guiding research funding for clinical trials.
tl;dr
We’ve recently published a new paper in Clinical Pharmacology & Therapeutics that looks at all the recent clinical trials involving cholesterol-modifying drugs. Specifically, we examined the differences between industry and non-industry funded trials in terms of their design. We wanted to know how the research agendas differ across the funding spectrum, and how that affects their contribution to comparative effectiveness research.
We found that industry-funded trials were more likely to compare between drugs (a surprise given what we know about published clinical trials), undertake larger clinical trials that finish sooner, less likely to examine cardiovascular risk, and less likely to measure safety outcomes.

Leave a comment